Shoulder arthroplasty, also known as shoulder replacement surgery, is a procedure used to relieve pain, improve function, and restore mobility in patients with severe damage to the joint. The surgery can be life-changing for patients suffering from arthritis, fractures, or rotator cuff tears. Just like hip and knee replacements, shoulder arthroplasty has become increasingly popular over the years as technology and outcomes improve.
 Shoulder anatomy
Shoulder anatomy
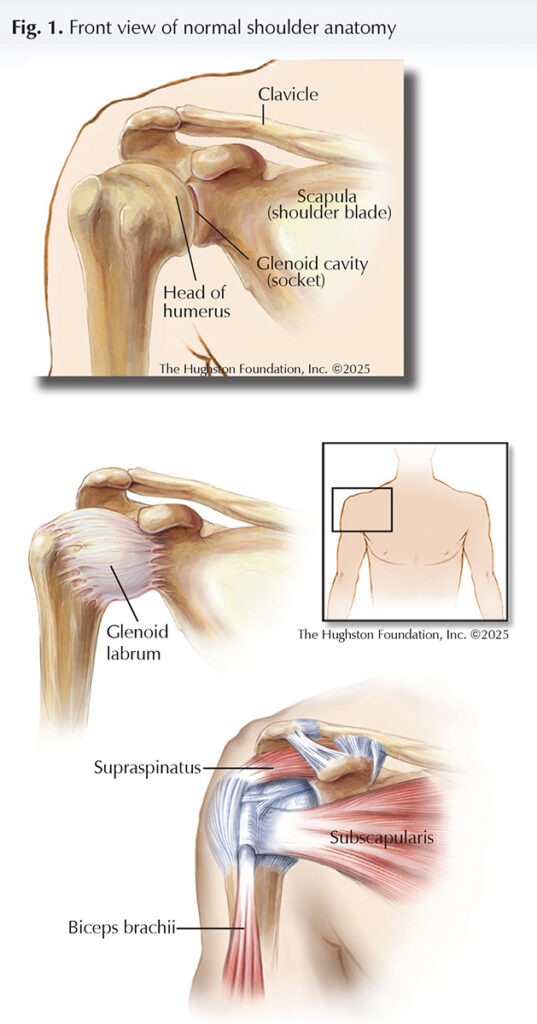
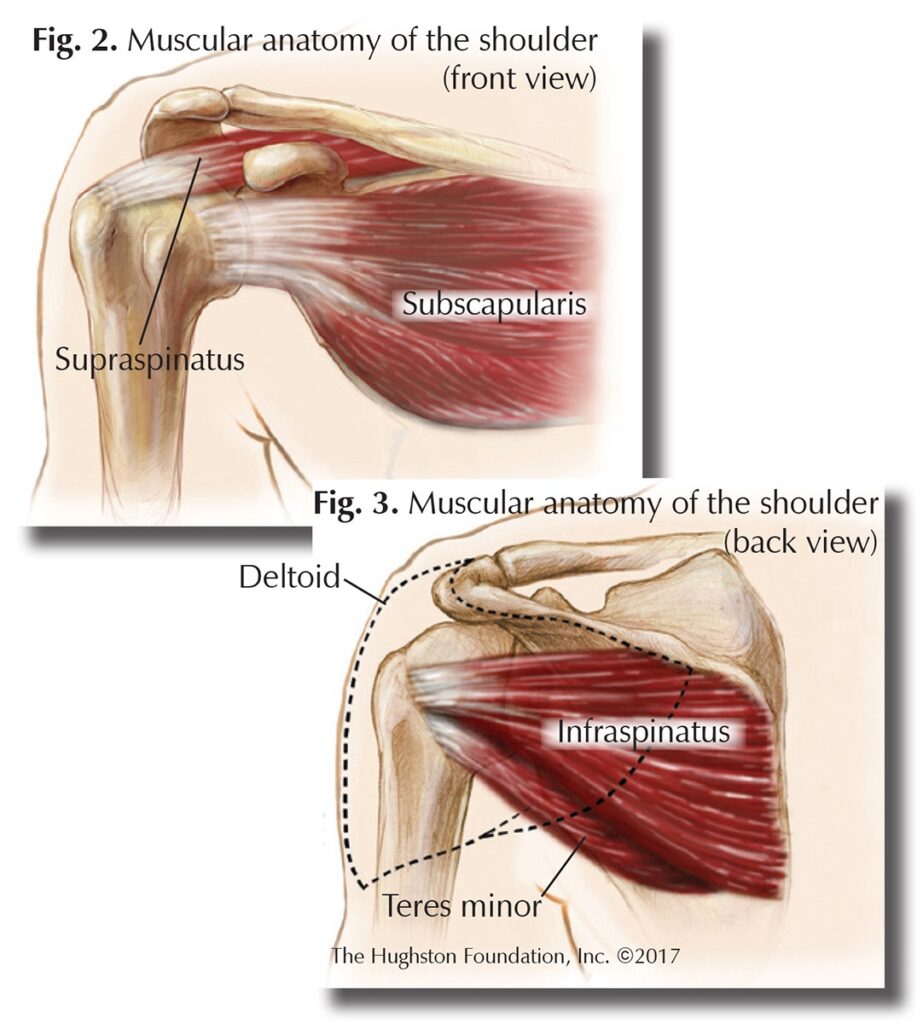
The glenohumeral joint, or shoulder, is a ball-and-socket joint. It is formed by the articulation of the head (ball) of the humerus, or upper arm bone, with the glenoid cavity (socket) of the scapula (shoulder blade) (Fig. 1). Since the cavity is shallow, there is little contact between the bones, but the glenoid labrum, a ring of cartilaginous fiber that lines its circumference, deepens the cavity by about 50%, allowing for a better fit. The joint capsule, which is the fibrous connective tissue that seals the joint space and provides stability, is very loose. This makes the glenohumeral joint the most mobile of the body, capable of flexion (bending), extension (straightening), adduction (pulling toward the body), abduction (pulling away from the body) medial and lateral rotation (turning toward or away from the midline of the body), and circumduction (moving in a circle). Because it lacks strong ligaments (tissues that connect bone to bone) to support it, the glenohumeral joint is a muscle-dependent joint. It is primarily stabilized by the biceps brachii, or muscle on the anterior (front) side of the upper arm, and the tendons of the supraspinatus, subscapularis, infraspinatus, and teres minor muscles that are called the rotator cuff muscles (Figs. 2 & 3).
Many factors can contribute to joint damage and pain, including trauma, disease, such as rheumatoid arthritis or osteonecrosis, infection, or chronic wear and tear resulting in osteoarthritis. The main indications for shoulder arthroplasty are arthritis, rotator cuff tears, and extreme proximal humerus fractures that cannot be surgically repaired or failed prior shoulder surgeries.
Types of shoulder arthroplasty
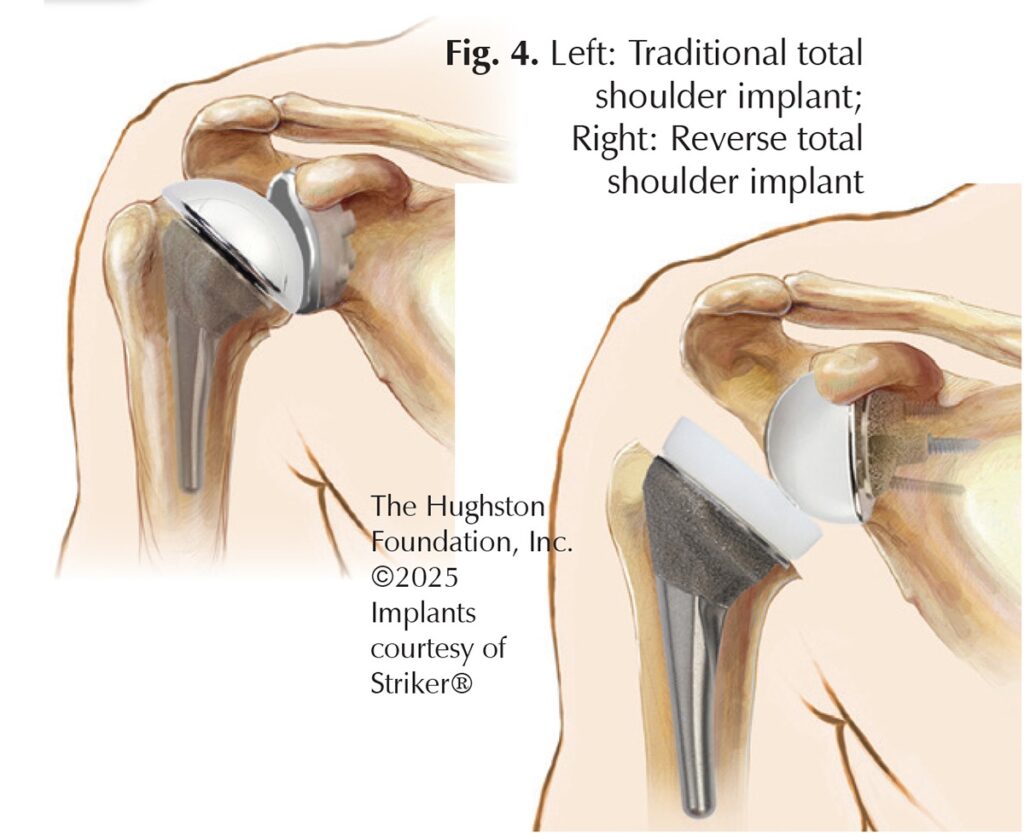 The 3 different types of shoulder replacements include total shoulder arthroplasty (TSA), hemiarthroplasty, and reverse shoulder arthroplasty (RSA) (Fig. 4). Total shoulder arthroplasty involves replacing the humeral head with a ball component and the glenoid with a socket component. It is ideal for patients who have an intact and functioning rotator cuff with good glenoid bone stock. Hemiarthroplasty involves replacing only the humeral ball of the joint with a component. It is ideal for patients with severe proximal humerus fractures, inadequate glenoid bone stock, or a deficient rotator cuff. Reverse shoulder arthroplasty includes replacing the humeral head with a socket component and the glenoid with a ball component. It is ideal for patients who have rotator cuff damage, elderly patients with proximal humerus fractures, and failed previous shoulder arthroplasty; however, it is essential to have a functioning deltoid muscle and axillary nerve to function properly.
The 3 different types of shoulder replacements include total shoulder arthroplasty (TSA), hemiarthroplasty, and reverse shoulder arthroplasty (RSA) (Fig. 4). Total shoulder arthroplasty involves replacing the humeral head with a ball component and the glenoid with a socket component. It is ideal for patients who have an intact and functioning rotator cuff with good glenoid bone stock. Hemiarthroplasty involves replacing only the humeral ball of the joint with a component. It is ideal for patients with severe proximal humerus fractures, inadequate glenoid bone stock, or a deficient rotator cuff. Reverse shoulder arthroplasty includes replacing the humeral head with a socket component and the glenoid with a ball component. It is ideal for patients who have rotator cuff damage, elderly patients with proximal humerus fractures, and failed previous shoulder arthroplasty; however, it is essential to have a functioning deltoid muscle and axillary nerve to function properly.
Surgical procedure overview
Surgeons perform shoulder replacement surgery under general anesthesia. The procedure can last anywhere from 1 to 2 hours on average. The surgical approach and type of implants used vary depending on the patient’s anatomy and other factors. During surgery, the surgeon removes the damaged bone and articular cartilage (covering on the ends of bones) and replaces it with prosthetic components.
Recovery
The postoperative hospital stay is dependent on the patient and the type of procedure performed. The recovery process is also patient-dependent and multifactorial. Typically, the patient’s shoulder will be immobilized in a sling or brace for a couple of weeks. Often, physicians prescribe physical therapy to work on passive or active-assisted motion during the early rehabilitation process, and then the patient progresses according to the postoperative protocol. Full recovery normally takes 4 to 6 months with continued improvements over a year.
Outcomes and prognosis
Most patients experience significant pain relief and improved function following shoulder arthroplasty. Long-term outcomes are favorable, especially with adherence to rehabilitation and activity guidelines. Modern implants’ survivability can last 10 to 20 years or more, depending on specific patient factors and use. Some patients may be limited in specific things like heavy lifting or high-impact activities; however, shoulder replacement is a practical solution to restore a patient’s quality of life that may have otherwise been limited by debilitating pain or loss of function.
Author: W. Cole Connelley, DO | Columbus, Georgia
Last edited on February 26, 2026